If a Calorie Were Just a Calorie, Then Any Weight Loss Program Should Work, Right?
No, not necessarily. There is a growing need to enhance the design of calorie-deficit meal plans by applying the mounting evidence in nutraceuticals. Providing nutrient-dense foods is part of the art of designing attractive menus that achieve the objective…weight loss. Now we have new insight on how nutraceuticals can be selectively added to meal plans to optimize weight loss.
Considering all the notorious weight loss plans, public health meal plans, fad diets and individualized diets used over the years, still, the latest World Health Organization (WHO) statistics on overweight and obesity remain staggeringly depressing. As of 2014 when WHO released global obesity statistics at 13%, a percentage doubling that of the 1980’s, nutritional interventions suddenly seemed paltry and ineffective at best.
Despite obesity being a result of a multifactorial system dysfunction, it is complicated at the heart of things by poor nutritional choices. While exercise is a critical piece of this multifactorial system, if nutrition does not lay a good foundation, problems with excess weight and the health-threatening inflammation the body suffers along with it will continue at the current startling rate.
Enter the 10 “game-changers” for optimizing any calorie-deficit plan. Including as many of these ten nutraceuticals can, by various mechanisms, set the physiological environment for losing weight, stabilizing blood sugar, controlling hunger, increasing insulin sensitivity, increasing thermogenesis and/ or affecting hormones regulating weight.
Optimize Your Weight Loss Plan Using These Nutraceuticals
While each of the following nutraceuticals may contribute a different percentage of benefit from small to large, adding even small percentage improvements together will equal a larger percentage of weight loss facilitation:
1. Probiotics. Two probiotics have been identified as contributing to a favorable environment for weight loss, Lactobacillus Plantarum, and Lactobacillus gasseri. Foods high in Lactobacillus Plantarum include sauerkraut, pickles, brined olives and some cheeses. It is also found as a prescription medication in some countries and as a supplement in others.
2. EGCG or Green Tea. EGCG stands for Epigallocatechin gallate, an abundant polyphenol found in its highest amounts in tea, specifically green tea and is used in many weight loss supplements. Originally thought to increase thermogenesis, it is now known that its effects lie more in interfering with the process of adipogenesis and it is the caffeine which is thermogenic. EGCG, in addition, acts in synergism with adiponectin, a protein hormone involved in glucose metabolism and fatty acid oxidation.
3. Psyllium Fiber. Although this fiber supplement has been used to relieve constipation in the past, recent research has shown it can also curb the appetite. If, when and how to use this nutraceutical must be individualized to the patient but remains an option as an appetite suppressant. Drinking a large glass of water with fiber added 20 minutes prior to meal should decrease the appetite and adding a feeling of fullness at mealtime.
4. Multivitamin. This is really a no-brainer, but any weight loss diet, particularly if under 1200 calories, requires a multivitamin to avoid deficiencies that may negatively affect energy metabolizing pathways.
5. Fucoxanthin. Technically, this is an antioxidant and one of the latest nutraceuticals to arrive on the supplement scene. It is classified as a carotenoid and is an extract of edible brown seaweed.
6. Chlorogenic Acid: Sold as “green coffee” and found in the flesh of peaches, eggplant, prunes and green tea is a phenolic compound.
7. Protein. Type and amount of protein may affect the rate of weight loss.
8. Capsaicin. Found in chili peppers, cayenne pepper, all peppers (except bell), it fights inflammation, acts as a fat burner, a performance enhancer and optimizes muscle growth.
9. Quercetin. A bioflavonoid found in onions, apples, kale, tomatoes, broccoli, asparagus or supplements of 150 mg. Works best with other bioflavonoids synergistically- such as green tea catechins.
10. P-synephrine. While obtainable through foods, it is safer taken as the extract. Previously thought to have cardiotoxic effects, these have been largely disproven.
Application:
By utilizing the above nutraceuticals to optimize nutrition plans menus can be developed that utilize foods and nutraceuticals that synergistically promote weight loss through one mechanism or the other whether it is decreasing appetite, interfering with fat metabolism, affecting the basal metabolic rate, providing the necessary nutrients for the body to burn fuel efficiently, promoting insulin and glucose metabolism or providing the optimal microbiome for weight loss to occur, such a menu approach should speed up safe weight loss while providing adequate nutrients along the way.
This information is not meant to diagnose or treat any condition. Rather it is encouraged that the assistance of a knowledgeable and trained weight loss professional be retained to travel this journey with you as you use these optimizers.
Nutraceuticals are extracts from food that have shown purported medical and/or nutritional value. Occasionally, nutraceuticals are used in the form of food, but the amounts needed are often too great to achieve the benefits obtained from the isolated food extract.
Because adherence to traditional diet and exercise programs is frequently challenging to many, there has been a fervent effort in the field of nutraceuticals to find compounds to assist this challenge. By adding a nutraceutical, hopes are that a more positive, rewarding weight loss in response to efforts will be seen, thus providing positive reinforcement to a continuation of efforts to achieve weight goals. Fucoxanthin is a nutraceutical that holds great promise in the wellness field, in general, and in the weight-loss industry in particular.1,2
Technically speaking, fucoxanthin is a xanthophyll and structurally like our good friend, Vitamin A, yet has no vitamin activity in the human body. It is present in edible brown algae and is the second most famous sea-based carotenoid, an antioxidant pigment also known to have many health benefits.3 Wellness Activity Profile of Fucoxanthin
Fucoxanthin has shown in both animal and human studies the following wellness activities:4,5
• Anti-obesity
• Anti-diabetic
• Anti-oxidant
• Anti-inflammatory
• Anti-cancer
• Anti-hypertensive
• Anti-lipemic Anti-Obesity Functions Identified
Many of these wellness effects are also relevant to each other, and, in particular, to anti-obesity. The beneficial effects of fucoxanthin identified that contribute to the alleviation of factors contributing to our global obesity problem include the following:
• Improvement in insulin sensitivity. 2
High insulin levels can lead to alterations in taste, perceived hunger, amount of food consumed and level of adipose tissue.
• Decreases blood sugar from a reduction in cytokine activity from white adipose tissue (WAT).
High blood sugar stimulates insulin production.
• Effects all 3 phases of fat deposition in adipose tissue decreasing overall the amount of fat stored in (WAT). White adipose tissue is more metabolically inactive than “brown” or even “brown” fat which have more mitochondria and are more thermogenically active than WAT.1
• May turn WAT into “beige” or “brown” fat 6,7 , although current studies on humans are controversial in this area.
Why would having more beige or brown fat cause increased rate of weight loss? Brown fat has more mitochondria than beige which has more mitochondria than WAT. Mitochondria are the power houses of the cell and are also responsible for thermogenic activity in adipose tissue.
• Increases Resting Energy Expenditure or thermogenesis. 8
Fucoxanthin has the unique capability of inducing “uncoupling protein-1 (UCP-1) in WAT’s mitochondria leading to the oxidation of fatty acids and heat production.
• Acts as an anti-inflammatory.3
Obesity is a disease of inflammation. Inflammation is a coordinated response to harmful stimuli, with the goal of returning the system back to a normal baseline. The inflammatory response triggered by obesity involves many components of the classical inflammatory response to pathogens and includes systemic increases in circulating inflammatory cytokines and acute phase proteins (e.g., C-reactive protein), recruitment of leukocytes to inflamed tissues, activation of tissue leukocytes, and generation of reparative tissue responses (e.g., fibrosis). However, the nature of obesity-induced metainflammation is unique compared with other inflammatory paradigms (e.g., infection, autoimmune disease) in several key aspects. The chronic nature of obesity produces a tonic low-grade activation of the innate immune system that affects steady-state measures of metabolic homeostasis over time.
• May increase the hormone adiponectin.3
Often deemed the “weight loss hormone”, adiponectin plays a huge role in regulating glucose levels as well as fatty acid breakdown.
• Activates AMPK.3,11
AMPK is an enzyme that regulates fatty acid break down, glucose metabolism, muscle oxidation of fat and sugar, inhibits lipogenesis (the creation of fat) and modulates insulin secretion, among other metabolic activities.
Studies on human subjects have shown a decreased weight circumference regardless of amount of weight loss, a decrease in liver fat, an increased responsiveness to chemotherapy, an increased metabolic rate and a decrease in body mass index with treatment of fucoxanthin. Safety Profile
Even though fucoxanthin is stored in the tissues for long periods of time (theoretically leading to overload or toxicity), no adverse symptoms have been noted in animal or human studies. Some concerns noted are the potential to consume excess iodine if fucoxanthin is consumed in large quantities from seaweed or kelp. While sufficient iodine is imperative to thyroid functioning, too much can be toxic to the thyroid gland and lead to its dysfunction. Food supplementation of fucoxanthin, however, has been shown to initiate weight loss, waist circumference and liver fat in healthy, overweight males.12 According to some resources, dosages of up to 2,000 mg/kg body weight were not able to demonstrate short-term adverse effects.3 Proposed Dosage
Suggested dosages from review studies and human trials range from 2.4 mg – 8 mg. 3,4,9 The benefits appear to be both dose and time related with the greatest effects on weight loss being seen after approximately 12-15 weeks of continuous daily dosing. The fucoxanthin, to be maximally effective, should be combined with a calorie-restricted nutrition plan with increased activity. Results seen with the combination effort will be greater than either intervention on its own. Summary of Overview
Pharmaceutical anti-obesity drugs are sparse, rarely effective for long and generally contain a laundry list of side-effects. Thus, the need for newer, safer anti-obesity agents are being fervently sought and studied with an increased emphasis on biologicals such as nutraceuticals.10
While obesity looms as a major threat to global health, to personal quality of life and as a precursor to life-threatening illnesses such as cardiovascular disease and diabetes, success with current weight loss interventions has been dismally unsatisfactory.
Clearly more human trials need to be done and this can be said of almost every nutraceutical and supplement on the market today. But, after reviewing the literature available on fucoxanthin as it stands today, this nutraceutical seems to be one of the most promising agents on the market today to help fight obesity and reward participants for accelerated outcomes for their work, thus increasing motivation in the long term to continue with the changes needed to achieve and maintain a healthy weight, BMI and percent body fat.
#fucoxanthin #obesity #nutraceutical #wellness Helpful Definitions: Adiponectin: Adiponectin is a protein hormone that modulates a number of metabolic processes, including glucose regulation and fatty acid oxidation. Secreted by the fat cells, or adipocytes, there is an inverse relationship between the levels of adiponectin and BMI. Leptin and Adiponectin have synergistic effects on hunger in the brain. AMPK. AMPK activation stimulates hepatic fatty acid oxidation, ketogenesis, stimulation of skeletal muscle fatty acid oxidation and glucose uptake, inhibition of cholesterol synthesis, lipogenesis, and triglyceride synthesis, inhibition of adipocyte lipolysis and lipogenesis, and modulation of insulin secretion by pancreatic beta-cells. Cytokines. are important in health and disease, specifically in host responses to infection, immune responses, inflammation, trauma, sepsis, cancer, and reproduction. Leptin. Considered the satiety hormone, leptin is a hormone made by adipose cells that helps to regulate energy balance by inhibiting hunger. Leptin is opposed by the actions of the hormone ghrelin, the hunger hormone. Nutraceuticals. Nutraceuticals are products derived from food sources that are purported to provide extra health benefits, in addition to the basic nutritional value found in foods. Products may show evidence of preventing chronic disease, increasing longevity, or to support the structure and function of the body. Technically, it nutraceuticals are not defined by US law, but generally refer to the noted definition here. Nutraceuticals are of pharmaceutical grade and considered a standardized nutrient. They are regulated as dietary supplements and food additives. References for Helpful Terms
Adiponectin. https://en.wikipedia.org/wiki/Adiponectin. Accessed 12/26/17
AMPK. https://en.wikipedia.org/wiki/AMP-activated_protein_kinase. Accessed 12/26/17
Cytokines. https://en.wikipedia.org/wiki/Cytokine. Accessed 12/26/17
Nutraceuticals. https://en.wikipedia.org/wiki/Nutraceutical. Accessed 12/29/17 References for Fucoxanthin:
1. Maeda H. Nutraceutical effects of fucoxanthin for obesity and Diabetes. J. of Oleo Science. 2015;64(2): 125-132.
2. Zhang H, Tang W, et.al. Fuxoxanthin: A promising medicinal and nutritional ingredient. Evidence Based Complementary and Alternative Medicine. 2015:20.
3. Examine.com. https://examine.com/supplements/fucoxanthin. Accessed 12/17/17
4. Wsiang T, Chi Jung T, et al. Efficacy of a low-molecular weight fucoidan as a supplemental therapy in metastatic colorectal cancer patients: a double-blind randomized controlled trial. Marine Drugs. 2017; 15(4):122.
5. Gammone M, D’Orazio N. Anti-obesity effect of the marine carotenoid fucoxanthin. Marine Drugs. 2015; 13:2196-2214.
6. Kwang-Min K, Sang-Man K, et al. The effect of Xanthigen on the expression of brown adipose tissues assessed by F-FDG PET. http:/dx.doi.org10.3349/ymj.2016.57.4.1038. accessed 1/3/18.
7. Rebello C, Greenway F. Fucoxanthin and its metabolites fucoxanithinol do not induce browning in human adipocytes. J. Agric. Food Chem. 2017; 65(50):10915-10924.
8. Orzio N, Gemello E, et al. Fucoxanthin: A treasure from the sea. Marine Drugs. 2012; 10:604-618.
9. Abidov M, Ramazanov Z, et al. The effects of Xanthigen in the weight management of obese premenopausal women with Non-alcoholic fatty liver disease and normal liver fat. Diabetes, Obesity and Metabolism. 2010; (12) 1:72-81.
10. Chu W, Phang e. Marine algae as a potential source for anti-obesity agents. Marine Drugs. 2016; 14:222.
11. Chang Y, Chen Y. Fucoxanthin attenuates fatty acid-induced lipid accumulation 0f Fx3B hepatocytes through regulated/AMPK signaling pathway. https://doi.org10.16jbbrc2017.11.022. Accessed 12/25/17.
12. Hall A, Fairlough A. Ascophyllum nodosum enriched bread reduces subsequent energy intake with not effect on post-prandial glucose and cholesterol in healthy overweight males: A pilot study. Appetite. 2012; 58:379-386.
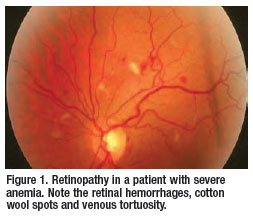
Anemia is (1) a deficiency of red blood cells in the body. The Red Blood Cells (RBCs) carry oxygen throughout the body. Symptoms of anemia are, most notably, fatigue, lack of concentration, mental fog, pallor. Other symptoms are feelings of discomfort or uneasiness, shortness of breath, and palpitations of the heart. Nails may become flat or concave. Anemia prevalence depends on many factors in both retinopathy and cancer (2), but is known to run as high as 80-100% in patients treated with chemotherapy.
Retinopathy is (3) an inflammatory condition affected frequently by circulatory problems. New blood vessels may grow on the surface of the eye. These blood vessels may cause vision to be spotty or blurry. This type of retinopathy is called “proliferative.” Retinopathy may also be present in those with diabetes as a complication of the disease in some individuals.
Having anemia or retinopathy decreases quality of life but treatments are available.
However, do we want to treat anemia of cancer and proliferative retinopathy? A study published by Dr. L.Smith in the February issue of the Journal of Clinical Investigation (5) indicates that treatment of anemia with erythropoietin, a hormone known to stimulate red blood cell production, which in turn, helps the anemia, may cause more harm than good. The findings by Lois Smith, MD, PhD, an ophthalmologist, concluded that the administration of erythropoietin may cause abnormal blood-vessel growth, thus complicating the treatment of anemia caused by cancer and retinopathy in mice.
Given at the wrong time, erythropoietin may make blood vessels grow and develop in the wrong manner. So, you might cure the anemia, but worsen the retinopathy. Erythropoietin when injected into mice, for example, caused numerous blood vessels to develop, but because the vessels were deformed, the retina was pulled to the back of the eye and the mice went blind. However, timing of the administration of erythropoietin introduced a study variable. When administered early, the disease process was slowed down. Administered later in the treatment the mice went blind.
This creates a dilemma in treating anemia. Now the question can be raised as to whether treating anemic conditions of abnormal cellular grown, such as cancer and retinopathy, with erythropoietin may yield anemic patients a worse fate. Will it make the tumors grow faster? Will it increase the rates of blindness? Clearly more research is needed with human subjects. Such treatment should now be followed to determine if abnormal cellular trends escalate with the erythropoietin treatments in human anemic patients.
Bottom line: This study does not yield enough evidence to say, “stop treatments of the anemias of cancer and retinopathy with erythropoietin,” but, monitor the literature, follow those patients more closely on a case study basis, conduct more studies in humans and introduce this study as a thought provoking variable when looking for evidence based research to back your treatment of anemia in these conditions .
A personal comment is about the nature of anemia. Let us not forget that while iron deficiency is the usual cause of anemia, we should never forget that B12, folic acid, B6 or protein deficiencies can all lead to anemia. Other causes of anemia include blood loss, inadequate production of red blood cells (aplastic anemia) or increased destruction of red blood cells (hemolytic anemia) that may present lifelong health problems. The causes, all causes, of anemia need to be identified and treated if a treatment plan is to be effective at meeting its outcome measures of alleviating the symptoms, the hypoxia and the anemia.
To provide the optimal nutrients for the thyroid gland to function while avoiding any drug-nutrient interactions from taking a thyroid replacement medication.
Function of the Thyroid Gland:
The thyroid gland is an endocrine gland that is normally located in the lower front of the neck. The thyroid gland makes hormones which are secreted into the blood and then carried to every tissue in the body. Thyroid hormones help the body use energy, keep warm and maintain the brain, heart, muscles, and other organs working properly.
What is hypothyroidism?
A low or inadequate supply of workable thyroid hormones due to many reasons. Here the focus is on simple hypothyroidism uncomplicated by any other disease entity such as an autoimmune condition.
Symptoms of hypothyroid:
May feel cold all the time, especially the hands and feet
Easily tire
Constant fatigue
Forgetful
Depressed
Weight Gain
Dry Skin
Hair falls out
Constantly cold, especially hands and feet
The first lab test doctor runs:
Thyroid Stimulating Hormone or TSH. If your TSH is >4.0 mU/L and your T4 level is normal, this may prompt your physician to test your serum anti-thyroid peroxidase (anti-TPO) antibodies for the autoimmune form of hypothyroidism. When these antibodies are present, it may indicate an autoimmune thyroid disorder, which is a risk factor for developing hypothyroidism. If you have these anti-bodies, your doctor will most likely perform a TSH test at least once per year. There is also ongoing debate on how to nutritionally support Hashimoto’, the autoimmune form of hypothyroidism, by not only controlling goitrogens, something to be discussed later, but by controlling food allergies as well. Hashimoto’s will not be discussed here.
So, what if my thyroid doesn’t function and it isn’t treated?
A goiter may develop. A goiter is a mass, an enlargement of the thyroid gland, that may choke the trachea (windpipe) and esophagus (swallowing tube) leading to symptoms, such as coughing, waking up from sleep feeling like you can’t breathe, and the sensation that food is lodged in the upper throat. A large goiter must be surgically removed.
Greater risk for birth defects
Heart problems
High blood sugar..diabetes
Fertility problems
Mental Health issues
High blood lipids
How can diet both prevent hypothyroidism and optimize thyroid function?
Obtain sufficient iodine intake. Iodine is required to make the first thyroid hormone, T4, the precursor to the active hormone, T3.
Table 1. Iodine Content of Foods
Life Stage
Recommended Amount
Birth to 6 months
110 mcg
Infants 7–12 months
130 mcg
Children 1–8 years
90 mcg
Children 9–13 years
120 mcg
Teens 14–18 years
150 mcg
Adults
150 mcg
Pregnant teens and women
220 mcg
Breastfeeding teens and women
290 mcg
In this case it is not true that if so much is good, more must be better. Too much iodine can be harmful, so don’t go overboard. Excess limits are listed below:
Life Stage Upper Limit
Birth to 12 months: Not established Children 1–3 years:200 mcg Children 4–8 years:300 mcg Children 9–13 years:600 mcg Teens 14–18 years:900 mcg Adults: 1,100 mcg/L
Obtain sufficient selenium in the diet so T4 can convert to T3. Selenium is needed in amounts of 45 mcg/day. Foods high in selenium include: butter, fish, garlic, sunflower seeds, Brazil nuts.
Table 2: Recommended Dietary Allowances (RDAs) for Selenium
Sardines, canned in oil, drained solids with bone, 3 ounces
45 64
Ham, roasted, 3 ounces 42 60
Shrimp, canned, 3 ounces 40 57
Macaroni, enriched, cooked, 1 cup 37 53
Beef steak, bottom round, roasted, 3 ounces 33 47
Turkey, boneless, roasted, 3 ounces 31 44
Beef liver, pan fried, 3 ounces 8 40
Chicken, light meat, roasted, 3 ounces 22 31
Cottage cheese, 1% milkfat, 1 cup 20 29
Rice, brown, long-grain, cooked, 1 cup 19 27
Beef, ground, 25% fat, broiled, 3 ounces 18 26
Egg, hard-boiled, 1 large 15 21
Puffed wheat ready-to-eat cereal, fortified, 1 cup 15 21
Bread, whole-wheat, 1 slice 13 19
Baked beans, canned, plain or vegetarian, 1 cup 13 19
Oatmeal, regular and quick, unenriched, cooked with water, 1 cup 13 19
Spinach, frozen, boiled, 1 cup 11 16
2. Obtain sufficient selenium in the diet so T4 can convert to T3. Selenium is needed in amounts of 45 mcg/day. Foods high in selenium include: butter, fish, garlic, sunflower seeds, Brazil nuts.
Table 4: Recommended Dietary Allowances (RDAs) for Selenium
Sardines, canned in oil, drained solids with bone, 3 ounces
45 64
Ham, roasted, 3 ounces 42 60
Shrimp, canned, 3 ounces 40 57
Macaroni, enriched, cooked, 1 cup 37 53
Beef steak, bottom round, roasted, 3 ounces 33 47
Turkey, boneless, roasted, 3 ounces 31 44
Beef liver, pan fried, 3 ounces 8 40
Chicken, light meat, roasted, 3 ounces 22 31
Cottage cheese, 1% milkfat, 1 cup 20 29
Rice, brown, long-grain, cooked, 1 cup 19 27
Beef, ground, 25% fat, broiled, 3 ounces 18 26
Egg, hard-boiled, 1 large 15 21
Puffed wheat ready-to-eat cereal, fortified, 1 cup 15 21
Bread, whole-wheat, 1 slice 13 19
Baked beans, canned, plain or vegetarian, 1 cup 13 19
Oatmeal, regular and quick, unenriched, cooked with water, 1 cup 13 19
Spinach, frozen, boiled, 1 cup 11 16
Milk, 1% fat, 1 cup 8 11
Yogurt, plain, low fat, 1 cup 8 11
Lentils, boiled, 1 cup 6 9
Bread, white, 1 slice 6 9
Spaghetti sauce, marinara, 1 cup 4 6
Cashew nuts, dry roasted, 1 ounce 3 4
Corn flakes, 1 cup 2 3
Green peas, frozen, boiled, 1 cup 2 3
Bananas, sliced, 1 cup 2 3
Peaches, canned in water, solids and liquids, 1 1
Carrots, raw, 1 cup 0 0
Lettuce, iceberg, raw, 1 cup 0 0
*DV = Daily Value. DVs were developed by the U.S. Food and Drug Administration (FDA) to help consumers compare the nutrient contents of products within the context of a total diet. The DV for selenium is 70 mcg for adults and children aged 4 and older. Foods providing 20% or more of the DV are high sources of a nutrient. The U.S. Department of Agriculture’s (USDA’s) Nutrient Data base external link disclaimer Web site lists the nutrient content of many foods and provides a comprehensive list of foods containing selenium arranged by nutrient content and by food name.
3. Avoid goitrogens for 4 hours after taking thyroid medication and some individuals do better avoiding goitrogens completely.
What are Goitrogens?
Goitrogen is a medical term that is used to describe any substance that interferes with function of the thyroid gland. The word itself comes from “goiter,” which means enlargement of the thyroid. If its ability to produce thyroid hormones becomes impaired, the thyroid gland can grow creating what is called a “goiter” in an effort to keep up with the body’s need for thyroid hormones.
How do goitrogens affect the thyroid gland?
Goitrogens, including soy, act on the thyroid by:
Blocking iodine:Goitrogens may prevent iodine from entering the thyroid gland, which is needed to produce thyroid hormones.
Interfering with TPO:The thyroid peroxidase (TPO) enzyme attaches iodine to the amino acid tyrosine, which together form the basis of thyroid hormones.
Reducing TSH:Goitrogens may interfere with thyroid stimulating hormone (TSH), which helps the thyroid gland produce hormones.
Goitrogenic substances, therefore, seem to have a negative impact on thyroid gland functions. Goitrogens are found in the following foods in high concentrations:
Broccoli
Cabbage
Kale
Cauliflower
Soy
Bok choy
Radishes
Cucumber
Rutabagas
Radishes
Brussel Sprouts
Spinach
Flax seed
Peanuts
For most goitrogens, varying your diet and taking precautions with these foods can make them less apt to interfere with the thyroid and to continue to provide the person taking thyroid medication the optimal benefits of treatment.
First, for all foods except soy, cook or blanch to break down the myrosinase enzyme which in turn reduces the amount of goitrogen.
Second, blanch all greens such as kale/spinach
Third, eat a variety of plant foods to limit the number of goitrogens in the regular diet.
These compounds interfere with iodine metabolism and inhibit thyroid hormone synthesis by blocking the formation of T4, the precursor to the active thyroid hormone called T3. Patients on Synthroid or other thyroid preparations should be cautioned to avoid or limit high goitrogenic food for optimal functioning of the medication provided to support the thyroid gland. Cytomel, another thyroid replacement medication, is extracted from the brains of animals such as pigs. People who do not respond to the artificial levothyroxine often end up on Cytomel. Problems with Cytomel include inconsistent dosage from lot to lot or pill to pill and potential transmission of prions (a genetically transferable infectious protein found in brain and nervous tissue of animals such as deer and cattle). Benefits are that it contains both T4 AND T3, no conversion is needed, and it is natural hormone.
4. Limit soy, a goitrogen, in diet and follow guidelines for goitrogens above for soy.
Now, speaking specifically on soy, according to Dr. Mike Fitzpatrick, an environmental scientist and phytoestrogen researcher, soy products can have a detrimental affect on both adults and infants. He believes that soy formula manufacturers should remove the isoflavones from the infant formula. This would be a clear example of preventive actions to avoid hypothyroidism. This, too, has been hotly debated with no clear guidelines put forth.
5. Vitamin/Mineral preparations are to be avoided 2-3 hours before thyroid medicationand 4 hours afterwards. Iron, calcium, magnesium, walnuts, soy, cottonseed meal or high fiber preparations specifically are to be completely avoided during this time frame. There are many other nutrients the thyroid gland needs including the macro-nutrient, protein. Developing a balanced nutritional plan following the guidelines herein and adhering to a balanced meal plan will promote wellness overall in general and to your thyroid gland, in particular. There are several nutrients that may interact adversely, so consulting a knowledgeable Dietitian may be useful or accessing The Natural Standards Database to search the interaction both may be useful in refining your nutritional program.
Regarding deficiencies, B12 is a common deficiency found in about 1/3 of hypothyroid patients.
Goitrogens are not limited to foodstuffs. Consider that the byproducts of cigarette smoking are goitrogenic as is Dilantin, an anti-seizure medication, and Lithium, a medication used to control mood swings in those who suffer from bipolar disorder.
The total number of goitrogens in the diet will determine whether and to what amount they will adversely interfere with optimal thyroid function, medication absorption and processing of necessary nutrients.
Application of Diet Guidelines
There is not enough education on how to take thyroid medication, so it can be absorbed effectively and thus aide the failing thyroid gland. Such things as taking medication on an empty stomach 20 minutes before food and 4 hours before any iron, magnesium or calcium supplements should be reviewed with the patient. Avoiding foods that inhibit absorption can help the thyroid function optimally, such as avoiding excess fiber close to medication time or consuming excessive goitrogens.
How much soy, a goitrogen, is safe? For infants, possibly none. This is a controversial area and more research is needed. For adults, just 30 mg of soy isoflavones per day is the amount found to have a negative impact on thyroid function. That would approximate 5-8 oz of soy milk, or 1.5 oz. of miso.
For infants born with a pre-existing low thyroid function, or put at potential for development of such, may be the most likely to suffer from the autoimmune form of hypothyroidism if they develop it later in life.
Other countries, however, are far ahead of the U.S. In July of 1996, the British Department of Health issued a warning that the phytoestrogens found in soy-based infant formulas could adversely affect infant health. They advised that breastfeeding be the primary method of feeding babies and if allergies to milk-based formulas were evident, then alternatives to soy-based formulas should be offered.
The bottom line again is we are all individuals. Some tolerate soy proteins just fine. Others cannot have it in their diet without problems. Once again, it takes a trained clinician to evaluate all factors in deciding whether soy is something to be avoided in your personal meal plan or not.
Further research on a Thyroid Diet for adults is indicated as well as further investigation into the effects of soy based infant formula on future development of auto-immune thyroid disease.
In conclusion, obtain adequate, but not excessive, iodine and selenium from foods preferably; avoid goitrogens as much as possible; if goitrogens are used in diet for their wonderful nutritional contributions, prepare them as outlined above to decrease effect of goitrogens; avoid during the time period before and after thyroid medication all substances listed in the hypothyroid diet; limit soy in diet and follow goitrogen guidelines when using it with medication.
Copy-write: Nutritional Synergy Handbook of Diets, Kathy J. Shattler, M.S., RDN
References and Bibliography
Devi RL, Chang HC, Doerge DR. Anti-thyroid isoflavones from soybean: isolation, characterization, and mechanism of action. Biochem Pharmacol. 1997. 54(10):1087-96
Filisetti TM, Lajolo FM. Effect of the ingestion of soybean fractions, raw or autoclaved on the rat thyroid. Arch Latinoam Nutr.1981.31 (2); 287-302.
Freake H. Iodine In: Stipanuk M, ed. Biochemical and Physiological Aspects of Human Nutrition. Philadelphia, PA:W.B. Saunders, 2000:764.
Forsyth WA. Soy protein, thyroid regulation and cholesterol metabolism. J. Nutr. 1995.125 (Suppl3):619S-623S.
Fort P, Moses N, Fasano M, Goldberg T, Lipshitz F. Breast and soy-formula feedings in early infancy and the prevalence of autoimmune thyroid disease in children. J Am Coll Nutrient; 9(2):164-7.
Jabbar MA, Larrea J, Shaw RA. Abnormal thyroid function tests in infants with congenital hypothyroidism; the influence of soy-based formula. J Am Coll Nutr. 1997. 16(3):280-2.
Kawicka and B Regulska-llow. Metabolic disorders and nutritional status in autoimmune thyroid disease. 2015.;69-80. Assessed 4/15/2016.
Klein M, Schadereit R, kuchenmeister U. Energy metabolism and thyroid hormone levels of growing rat in response to different dietary proteins – soy protein or casein. Arch Tierernahr 2000. 53(2);99-125.
Soni M, White LR, et al. Phytoestrogen consumption and risk for cognitive decline and dementia; With consideration thyroid status and other possible mediators. The J of Steroid Biochemistry and Molecular Biology.2015. Accessed 4/15/16.
Wan Y and E Crosbie. Soy intake and endometrial cancer risk varies according to study population. BLOG. An International Journal of Obstetrics and Gynecology. 2014. 122:311: doi: 10.1111/1471-0528.12859. Accessed 4/15/16.
Note: Drug-Nutrient Interaction between Levothyroxine and Nutrients
Drug-nutrient interaction handbook by Pronsky, et al, 2015, with the following precaution listed: “soy protein may cause an interference in the absorption of thyroid medication” and cautions “if soy is to be consumed that it be consumed 4 hours after taking the thyroid medication. “It goes on to say “Take Fe, Ca or Mg supplement separately from drug by >4 hours. Decreased absorption reported with soy, soy milk, soy infant formula, walnuts, cottonseed meal and high fiber foods as well as grapefruit and citrus.”
After reading several “trending nutrition articles” on “hot” topics for this year, one glaring trend stood out . . . the outstanding lack of trust on the part of the public on advice from so-called “experts”, the same experts who are known to disagree with each other on a regular basis despite a commitment on their part to “evidence based practice.” We have lost the public’s trust. It is our fault. We stand guilty as accused.
In some respects, has the public put too much trust in achieving consistency in information? Instead of striving for consistency, perhaps we should be honoring the intuitiveness of the art of practicing any form of medicine. Since all humans are different, studies cannot be consistent and individuals cannot be treated the same while we claim we practice “personalized medicine”.
The truth of the matter is nutritional medicine is an art and a science. Part of the art in nutritional medicine is to see the picture in its entirety and to be able to explore different approaches to fitting the pieces of the puzzle together to optimize outcome. The combination of research, evidence, observation, intuition – all are used in various alternative as well as traditional forms of medicine and used effectively.
The key to making this happen is in the clinician’s knowledge base, experience/foundation in nutritional medicine, critical thinking skills and respect for every patient as an individual, as a unique biochemical entity with a unique microbiome, need for nutrients, potential for supplement-drug interactions, genetic tendency towards chronic disease, etc.. all this while considering the most updated Evidence-Based Guidelines of Care for that particular problem area- be it Cardiovascular or Diabetes. Defining the Field
What is a “nutritional medicine” approach? In today’s world, it no longer means a rejection of synthetic drugs and treatments, but a more complimentary approach where diet and nutrition, fitness, environment, among other synergistic factors, are used to enhance medical treatment. Most diseases in the mind of the nutritional practitioner are caused by years of unbalanced nutrition and even when genes are involved oftentimes it is a poor lifestyle that enhances the expression of those genes.
Not to confuse the practice of nutritional medicine with the practice of medicine, let’s clearly delineate the differences. The practice of “medicine” is defined in the Merriam-Webster dictionary as “ the science and art dealing with the maintenance of health and the prevention , alleviation or cure of disease; a substance used in treating a disease; the branch of medicine concerned with the nonsurgical treatment of disease.” Taber’s Medical Encyclopedia defines it thusly: 1) A drug or remedy; 2) The act of maintenance of health, and prevention and treatment of disease and illnesses; 3) Treatment of disease by medical as opposed to surgical means. None of these are specific to nutrition. Traditional doctors average one nutritional course in their heavy curriculum.
The definition of “Nutritional Medicine”, on the other hand, explains the field thusly:
1. The use of food and nutrition as a medical approach.
2. Supplementation of diet with nutrients, intermediary metabolic products and probiotics to prevent illness and improve health and disease.
3. The study of the synergistic interactions of a variety of factors such as environment, social health, physical health, fitness, spiritual health, physiology, anatomy are all considered in relation to the nutritional status and needs of the patient. The nutritional medical approach is based on a wide range of disciplines with a focus on application of the knowledge of foods, nutrients, metabolism, counseling, education, medical nutrition therapy and behavior change.
And, finally, in 2005 the definition in Elsevier Jones Mosby’s Dictionary stated that nutritional medicine was 1. Use of food and nutrition as a medical approach and 2. Supplementation of diet with nutrients, intermediary metabolic products and probiotics to prevent illness and improve health and healing. Medical Nutrition Therapy (MNT) is the term we use for the arm of nutritional medicine that deals specifically with the aspects of nutritional care delegated to Dietitians (a title protected term) who meet practice qualifications as discussed later. To put nutritional medicine back at the forefront of importance in the healing process, doctors can and should make use of Registered Dietitians, the professionals that now specialize in the area of nutritional medicine and are most trained to be the doctor’s greatest ally for patient education, behavior change and positive nutritional/lifestyle outcomes.
Regaining the Trust of the Public
The first step in regaining the trust of the public is to talk openly about what nutritional medicine is and provide education on what to look for in a doctor, nutritionist or even in reading material– especially while cruising the internet highway- to determine credibility.
Next, to regain trust explanations on how this has happened in the first place needs to be identified, explained and rectified. Becoming a savvy nutrition consumer is a necessity these days for everyone. What are some things to look for?
Look for credentials to indicate that a minimum level of education/experience/testing have been conducted to verify the professional is properly trained to provide reliable nutritional information that is up to date and individualized as appropriate.
For dietitians, they should be licensed in states of licensure and credentialed in states without licensure.
Doctors may exhibit additional training in the nutrition sciences
Doctors may be of an integrative and functional medicine philosophy with accompanying credentials
Check to see licenses are valid with the state
Look at references, testimonials, ratings
Contradictions Everywhere, Who to Believe?
The contradictions in information the public complain about is very real. Here are some of the reasons why:
It seems like everyone is a “nutritionist” including fitness trainers, retail supplement clerks, grocery store clerks, nurse assistants, any weight loss program consultant, and those in the news media. Not one of these nutrition information gurus average any more than zero to one course in nutrition at best.
The Federal Government seems to be at the root of much confusion. For example, the 2011 Recommended Dietary Intakes are not in agreement with the 2015 DietaryGuidelines. The outdated ATP (Adult Treatment Panel Cholesterol) III guidelines are contradictory to the new American College of Cardiology (ACC)/American Heart Association Cholesterol Guidelines in 2013 (designed to replace the Adult Treatment Panel III –ATP). Great debate ensued and the outdated ATP guidelines are still being used 14 years later. The 2013 Guidelines put out by ACC/AHA were then challenged by the National Lipid Association (NLA) with different guidelines for cholesterol and lipids being reissued in 2015. The AHA/ACC guidelines of 2013 relative to diabetes were rejected in a 2015 publication of Cardiovascular. Now, can you see how difficult it can be for trained professionals to sort out all of this contradictory “evidence” and to keep up with it as it changes, studies come to conclusions and guidelines are revised?
Nutritionists are not without blame either. In 2016 within minutes of each other a study was released stating we were in a Vitamin D pandemic while a study in Lancet suggested lowering the limit on Vitamin D need and what is “technically” considered the upper limit. The studies, conclusions and recommendations were totally opposite of each other.
Many writers draft their information without checking their sources or knowing how to check a source. Findings frequently come out of poorly designed studies with too few subjects, subjects all of the same sex, no control group or replicability, etc. and are not fit to generalize in a 6 pm news segment to the rest of America.
We can’t take the art out of science or there would be no such thing as a “second opinion.”
And, just because a medical doctor is an M.D. or a D.O. does not mean they are trained in nutritional care, either.
Furthermore, every Registered Dietitian, just like doctors, operate from their own philosophical platform when it comes to running their practices. Just as human beings are all biochemically individual, so should the treatment be. There is no “one size fits all” answer despite the push for that ONE consistent piece of nutritional truth.
So, with that said, what types of credentials should you look for in someone practicing as a Nutritionist? Credentials
By this point, hopefully, it is understood that even with the guidance of skilled practitioners it is difficult to find one standardized answer to a medical or nutritional question. Practitioners are trained to accept the guidelines that meet the approval of the majority and with the greatest strength of evidence utilized. That is, if they have time to keep up with the changing guidelines while maintaining a busy practice.
Most U.S. and many foreign physicians have one nutrition class and many do not pass graduate level biochemistry classes. Probing to see what type of advanced study a physician has had or what their views are on integrative and functional medicine may give you a clue as to the extent of their skill in nutritional management.
With all due respect to physicians, many are not trained to deliver nutritional services and some cannot even identify the need for such. Others come with a respected background in Alternative and Complementary Healing practices such as Ayurvedic Medicine, a practice centuries old and well respected in many countries. So take care not to be too judgmental, just do your research. Information on complementary medicine may be obtained by the National Center for Complementary and Integrative Medicine , a U.S. Federal website.
With nutritionists, credibility has become more cut and dry in states that have licensure. In most states licensure protects the public by not allowing individuals to practice “Dietetics” or call themselves Dietitians or Nutritionists without meeting the same criteria that all Registered Dietitian Nutritionists (RDNs) have to meet:
1. Obtain a minimum of a Bachelor of Science Degree that includes a core curriculum of classes approved by the Commission on Dietetic Registration. These classes include foods, food management, nutrition, statistics, counseling, professional literature, microbiology, food service management, menu planning, pharmacology, chemistry, biochemistry, physiology, anatomy, to name just a few. In the near future a Master’s Degree will be required to become an RDN and to sit for the National Board Exams.
2. A supervised 900 hour internship;
3. The successful passing of National Board Exams;
4. The maintenance of 75 continuing education credits every 5 years
This qualifies the practitioner to be an Entry Level practitioner as opposed to Competent or Expert. These categories are based on additional education, certification and experience.
Not all licenses are held by RDs, but all licensees must meet the minimum qualifications above, so Dietitians essentially are setting the Gold Standard for minimum criteria for licensure by any other profession than an RD or RDN.
Now, not even all highly qualified RDs agree. It involves their level of specialization, what theory they practice by, their experience in specific areas and how duped they have become by the contradictory nature of published studies and under-researched news stories.
But, if someone were to take the chance on listening to a clerk with a high school education or listening to a skilled practitioner with critical thinking skills and constant competency testing, who do you think you should believe? Who Does What These Days?
When the dust settles, things will be much different in who practices what. It is in the scope of practice for the “qualified” Dietitian to practice Medical Nutritional Therapy. Medicare now allows Dietitian’s to write diet orders, order supplements, order nutritional labs to follow up on nutritional intervention, perform the nutritional teaching and follow the patient without the doctor’s orders and solely based on the RDs competency level and the admittance to the Medical Staff. RDs are uniquely prepared to handle all aspects of nutritional care.
In some states Dietitians operate private practices similar to Physician’s Offices. Physicians still need to order consultations for many insurances to pay for outpatient visits, but not so in the hospital setting any longer.
So, in a U.S. hospital if a patient has nutritional needs it is the law that they be seen by a “qualified” dietitian, not a diet technician or a physician, but a qualified dietitian. If this does not occur, the hospital is in violation of Joint Commission rules. This is said with emphasis because too many malnourished patients and patients with complications are being readmitted time and time again for the same problems because hospitals have not implemented the new Medicare rulings and patients don’t know when to push for their rights AND nutritional needs are not being met in far too many scenarios.
This is a huge change in the face of nutritional care. What started out as the mainstay of medicine was forgotten with the dominance of the prescription pad and then reborn like a rising Phoenix in Dietitians. What doctors don’t have time to do has now been delegated to RDs, RDNs, and Registered Nutritional Technicians (RNTs), most members of the national organization Academy of Nutrition and Dietetics (AND).
So, in summary, what does the changing face of nutritional medicine mean to the public? It means doctors have trained/qualified assets to use to assist them in implementing the nutritional orders they give to patients. . . . to change their diet,to follow a special diet but no instruction or training provided, lose weight, exercise, eat better, lower the blood sugar, decrease the blood pressure, and eat less sodium. It is the RDs that are the ones that help patients figure out how to follow the doctor’s orders, which calcium supplements to take and how much, how to implement public health guidelines, and, in general, to assist the public in questions regarding supplements or drug/supplement interactions.
So, as a result, doctors are more aware of the growing evidence-based importance of nutritional medicine, but just don’t have the time and/or training to work implementing the plethora of nutritional teaching needed. It is the Dietitian’s job to help the Doctor optimize his practice of nutritional medicine by teaching patients and the public on preventive health and nutrition for disease prevention as well as to optimize medical treatment in the treatment of the disease process.
So, in essence, look for doctors that respect the statement by Thomas Edison “The doctor of the future will no longer treat the human frame with drugs, but rather will cure and prevent disease with Nutrition.” That time is here. Now. And so are RDNs.
**Caution with State Laws as many are ten years behind actual reality. Maintain malpractice insurance, be friends with attorneys and the healthcare playing field is about to get very different.
Reference: Academy of Nutrition and Dietetic. http://www.eatright.org. Accessed 4/30/16
Davies S. 1991. Scientific and ethical foundations of nutritional medicine. J of Nutr Med 2; 227-247
ACC: American College of Cardiology
AHA: American Heart Association
AACE: American Academy of Clinical Endocrinology
AND: American Academy of Nutrition and Dietetics
NLA: National Lipid Association
ATP: Adult Treatment Panel
CDR: Commission on Dietetic Registration
RDN: Registered Dietitian Nutritionist
The Weight-Loss Supplement Question That Just Won’t Go Away, and that is the way it should stay!
The question: I am taking a weight loss supplement called OxyElite Pro and am wondering if it is a safe choice for me?
The answer to this question was quickly found in the international archives of the academic and popular internet entanglement. And why is it said that the question should always be asked about weight loss supplements? Weight loss supplements are largely unregulated and have been known to contain ingredients that aren’t on the label such as prescription medications, to contain ingredients that could harm or even kill the consumer, the supplement doesn’t contain any of the active ingredient it says it does, or among other reasons not stated here, it may be contaminated with lead or other harmful substances. Before taking any supplement claiming to product weight loss, a health care professional such as a doctor or Registered Dietitian (RD) should be consulted – it might just save your life!
What does the research say about OxyElite Pro?
“OxyElite Pro is a fat burning supplement sold by USP Labs. Until 2013 it contained DMAA, an illegal stimulant drug linked to cardiac arrest, liver failures and death. After it was reformulated with more unapproved ingredients, it was linked to a deadly outbreak of liver damage. In February of 2015 the FDA lab tested the antidepressant Prozac in “Oxyelite Pro”. Schmidt Law Firm
Questions from a curious public started pouring in from all over the globe about this supplement that many have heard about, or know it by different names, but with the same offending chemical –DMAA, technically 1, 3 dimethyamylamine. A few years back a weight loss supplement called Oxy-Elite Pro came to the forefront of the Food and Drug Administration’s (FDA) attention due to over 100 reports across 16 states of hepatic and cardiovascular complications, transplants, and even death. These reports were traced back to Oxyelite Pro and the DMAA it contained. The product was reported as being recalled by the FDA.
This same weight loss supplement, after remarketing, was reported as containing DMAA hidden under various names related to the geranium plant, and were caught again. The company took out DMAA, or seemingly worked out its legal issues, and replaced DMAA with Higenamine. At first blush, this appeared to be a safer alternative. However, after researching Medline and google scholar it was shocking to find that higenamine had not been orally tested on humans, only rabbits, until a small and poorly designed study in 2013.
We have nothing to guide us to therapeutic amounts of Higenamine, toxic amounts, side-effects, drug-interactions. We do know Higenamine acts as a blood thinner, anti-inflammatory, has been known to deplete dopamine levels and acts in a similar manner as ephedrine and synephrine. Anyone up for a drug interaction???
Whether counterfeit or not (as some dubiously claim), it doesn’t stop there. The FDA announced in February of 2015 that Prozac, a prescription antidepressant, had been found in international shipments of Oxyelite Pro. Prozac is a selective serotonin uptake inhibitor or an SSRI. If someone takes another SSRI and is already on an SSRI from their doctor, a life-threatening condition called Serotonin Syndrome may develop.
What does this fascination with Oxyelite Pro mean to Doctors, RDs and Nurses? We need to be diligent in teaching our fellow clinicians about this product and the chemical names causing problems and why.
Now there is the question of scope of problem. How many people with chronic illnesses get worse, or even die, from taking products made by companies that just can’t seem to get it right? What do we do if our opinion is asked? How many clinicians have the time to go to google scholar, Medline, Natural Standards Database, and the FDA webpage to answer a question? I do know from experience that products banned in US were still being used and approved of by physicians in India. I do know that it is back on the market with thumbs up at the FDA.
Researching products for customers is very time consuming and costly to the clinician. Look towards resources to help expedite the provision of accurate information to consumers such as from Examine.com or Natural Standard Database, Google Scholar, FDA. A recent FDA release on Oxyelite Pro may be found at:
Contrary to some misconceptions, RDs can recommend supplements. In fact, RDs credentialed in certain states can order diets, lab tests, supplements and IV TPN solutions. Many do anyway as it is in our scope of practice and depends on the RDs level of competency, skills and in consideration of state law.
One of our biggest responsibilities is advising consumers about weight loss supplements, benefits and risks. OxyElite Pro is a supplement worth knowing about. And, the ingredients DMAA, geranium oil, and higenamine are 3 ingredients to think twice about before making that supplement choice.
Weight Plateaus are those frightful, bothersome states of metabolic stagnation that occurs smack dab in the middle of a successful weight loss plan. Even if expected, plateaus are cause for discouragement, feelings of failure and a desire to “give up”.
No, no need to give up. Let’s look at some game changers for those plateaus
At the bottom of this physiological storm is that of survival. In a plateau the body is fighting to stay alive, so it lowers its metabolism to match the calories being given it. Yes, it defeats the purpose but the body is just trying to save its own life by this metabolic shift. The question(s) then become the following:
Do we reduce calories further?
Do we take products to increase the thermogenesis back up to normal?
Do we manipulate the diet to confuse things?
Do we manipulate the energy output through the exercise routine?
Do we take a step further into analysis of our relationship with food?
Knowing now the factors to be dealt with in permanently dealing with plateaus, let’s make a little toolbox of things that will help increase energy expenditure while working with calorie manipulation.
Plateau Interventions, What Should be in Your Toolbox????
Meal Plan Manipulations
Keep the Food/Symptom Diary again if you are not still doing it. Sometimes, as the same old regimen is repeated, boredom slips in. Calories begin to creep back in, portion sizes aren’t watched like they used to be. Go back to the basics: weigh, measure and revisit portion sizes and food choices.
Intermittent-Fasting Routine: For this plateau buster, the weight loss is facilitated by moving calories. For 2-3 days either a very low calorie diet (800 calories) or a fast can be chosen to throw the body’s expectations off. Do this for two days then go back on your meal plan for 3 days and then fast or follow a very low calorie diet on an every- other- day basis. There are various renditions of this manipulation. Now, hunger is still a problem with this type of plan unless your fasting days take you into ketosis. Not appropriate for diabetes.
Fasting is associated with increased ghrelin and decreased obestatin in the blood circulation. Specifically these naughty hormones are ghrelin and obestatin. Both hormones play intricate roles in playing with our regulation of diet induced thermogenesis,
Calorie-Restricted Adequate Nutrition (CRAN): This meal plan, originally developed in life- extension research, was found to be effective at keeping the body lean and mean, but it is not practical to live on such small amounts of food with supplementation for extended periods of time. These human studies continue, but now the rage is to look for CRAN mimetics that make life more livable. However, short term use can blast a hole in a plateau!
Macronutrient Manipulation: Take your meal plan and flip flop it. For example, low carbohydrate high protein for one month may be different. Some meals will be turned from a meat based to a vegetarian based or from a regular carbohydrate diet to a low glycemic carbohydrate, high protein diet. Again, your body is fooled for a bit.
Then, don’t forget the little plateau “busters”: a) drink 8 oz. glass of water or sugar free beverage prior to a meal; b) achieve adequate hydration, but not too much – 1 ml per kcal or 8 glasses per day and consume high water foods such as melons, hot cereals; c) keep your sodium to the recommended level of 2,300 mg. sodium/day or higher if exercise requires it.
Exercise and Lifestyle
Change Your Workout Routine: Keep your metabolism guessing! Here are some guidelines creating new work-outs for your toolbox. Have fun with the following ideas!
Redesign your old work –out program by changing one or more variables – frequency, intensity, duration.
FREQUENCY: Change the number of times you do a work out per week
DURATION: Change the length of time you do a specific workout
INTENSITY: Increase your target heart rate for 20 minutes of the cardio portion of the routine
Add Yoga or Tai Chi to your routine – pay attention to breathing exercises and isometrics
Use Video exercise programs to increase compliance
Try to get fresh air and walk daily!
Remember to adjust your fluid and meal intake to the type of sports you are in – professional athlete vs. weekend warrior.
Get in touch with your hunger signals again and what that feeling is like.
Plan ahead for parties and social events.
Thermogenic Aides
or
Where’s the Pill?
A pill is not our long-term answer. Short-term like in Breaking a Plateau, it is reasonable.
And, our top contenders for Thermogenic Aides are:
Green Tea: This herb has been used medicinally for a very long time. Studies have shown that green tea can help reduce obesity when consumed on a daily basis. I seems to work by increasing metabolism after eating. Green tea may also reduce the appetite, fat absorption and storage. To break a plateau, drink 6 0z of caffeinated green tea 3x per day until weight loss established again.
The chemicals responsible for green teas effect on weight are primarily from ECGC, catechins and polyphenols
Green Tea should be respected as a known adjunct to reducing the BMI, body weight, body fat, reduction of overall fat cell generation, decrease in fat absorption and in the suppresses of appetite
Hot, Spicy Foods: Incorporate the use of hot chili peppers and turmeric in meals. These spices cause a slight sweating reaction and a greater response to the food thus elevating thermogenesis.
Resveratrol: Resveratrol has been on the market for many years and has been used medicinally for generations. Controversial human trials continue, but studies have shown that 150 mg of trans-resveratrol will cause weight loss in obese but not normal weight humans.
Vitamin D/Calcium: Approximately 90% of our world’s population is deficient in vitamin D. Vitamin D is actually a hormone and recent reports suggest our rise in obesity is related, in part, to our lack of Vitamin D and Calcium
Bitter Orange, p-Synephrine, Caffeine, Kola Nut: These nutrients/foods- all thermogenic teas-can be
used alone or in combination to break the plateau. No adverse side effects have been found.
Vitamin C: Vitamin C is inversely related to body mass. Individuals replete in vitamin C oxidize 30% more fat during moderate exercisers than those who were depleted. Dosage should be 250 mg by food (preferably) or supplement.
Transformation of our Mindset
Change your mindset – see yourself as you want to be, see yourself as you wish to look. This is best done in a state of meditation or prayer
Mentally visualize how you will handle challenges you know may tempt you and be ready for them. The more you practice your responses the easier it will become.
Positive Self-Talk (I look good today or I feel good, what a beautiful morning)
Increase use of support groups ( they can help push us through challenging emotional times that lead to overeating)
Self-hypnosis
Add a buddy system
Accepting and anticipating challenging weight plateaus will either encourage success as each plateau is out-witted or you accept defeat. So, take the challenge and win, out-win that plateau! Once the energy level is restored and the pounds start coming back off again slowly start back on your original (or revised) meal plans and exercise routines.
In taking an Integrative and Functional Medicine Approach, we must look at our tool box holistically. Approaching a problems from many angles means utilizing the most neglected tools to meet our goals at all levels the problem.
Singh R. Significant improvement in obese, grade three male individual with nutrient dense low calorie, moderate to high protein diet. Advances in Obesity, Weight Management and Control2015. 2(2)
Stohs SJ, Preuss HG, and Mohd Shara. A review of the human clinical studies involving citrus aurantium (Bitter Orange) Extract and its primary protoalkaloid p-synephrine. International Journal of MedicalSciences 9(7): 527-528. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3444973/ Accessed 5/22/15.
Timmers S, Konings E, Bilet L, . . .Calorie restriction-like effects of 30 days of resveratrol supplementation on energy metabolism and metabolic profile in obese humans. Cell Metabolism. 14:612-622
It had to happen sometime . . . health professionals don’t agree with the evidence that created guidelines that we are to follow as standards of care. What happened? No one seemed to notice as the American College of Cardiology/American Health Association released, with the blessings of the National Heart Lung and Blood Institute, the 2013 guide on Cholesterol, the guide to replace ATP III.
Ignored was the fact that guideline ES16 confidently stated that limiting dietary cholesterol did not have sufficient evidence to continue advising individuals to limit it in their food.
In fact, in the cardiovascular section of the Nutritional Care Manual (NCM), it still advises a restriction of dietary cholesterol to less than 200 mg/day. They also continue to recommend a diet distribution of 25-35% fat when the 2013 ACC guideline number ES11 states that a diet restricted in fat to 26-27% fat has the greatest positive effect on lipid reduction. The Academy of Nutrition and Dietetics, who profess to practice by evidence based medicine and publish the Nutrition Care Manual, have been caught not upholding the very standards they ask us RDs to uphold. The NCM manual has not added the revised Asian BMI of 23 to our Assessment Criteria for the cardiology section, they ignored the % dietary fat distribution recommendation and they ignored the updated cholesterol guidelines.
Cholesterol restriction can deplete our choline, a conditionally essential nutrient, to levels that can precipitate a deficiency. Cholesterol makes up a good share of the brain and the tissue making up our nervous system. That is one reason why blood cholesterol will traditionally go up in pregnancy as the fetus needs the cholesterol for brain and nervous system development.
Then today I opened my mail to find an article by David Templeton on how Scientists Debate the Impact of Removing Risk for Dietary Cholesterol. It took us two years to realize a change had been made? This is called “being on Top of Things”. The researchers had ten years while everyone waited for ATP IV (which never came, just the 2013 ACC guidelines), to collect the data needed to make a decision on dietary cholesterol, but I guess no one was interested.
Quite a conundrum isn’t it? To have therapies that work, but we shout “Where’s the evidence?” and to have no evidence and complain because the lack of evidence changes our intuitive way of treating our patients?
I can see both sides of it as I lean towards integrative medicine. There are many therapies in integrative medicine we don’t have “evidence” for but work. So, to be true to ourselves what is it going to be? Pick and choose the evidence to follow? Is that being true to a commitment of “evidence based practice”? And, for those organizations professing evidence-based practice, what is the responsibility of that organization in keeping the stakeholders up-dated as to current evidence? What timeline should they set for themselves, two years? Is that reasonable?
Let’s take a look at the gastric bypass and blood sugar control . . .
Almost 80% of patients who undergo gastric bypass surgeries to lose weight show abnormal glucose tolerance when administered a glucose challenge. Some patients are downright hyperglycemic to the point they could be diagnosed as diabetic according to a news release from the American Society of Metabolic and Bariatric Surgery meeting awhile ago.
The working hypothesis, according to researchers, is that there is an enhanced insulin response which triggers low blood sugar with a corresponding increase in appetite. The rapid emptying of the gastric pouch is more than likely the cause for the enhanced insulin response. The combination of the rapid emptying of the pouch and low blood sugar are causes for increased appetite.
This finding has raised questions regarding whether the gastric bypass should remain the gold standard for weight loss for the morbidly obese. At the very least, it was suggested that a valve be inserted in the bypass procedure.
Patients are alarmed at the rapid increase in weight and surprised at the ravenous appetite that develops so soon after a meal.
Sixty-three patients were clinically studied who had undergone gastric bypass procedures. All the patients had a 100 g glucose tolerance test where the glucose was measured one and two hours after a meal. The investigators defined low blood sugar as less than 60 mg/dl or a decrease of 100 mg/dl or more within two hours of a meal challenge and no glucose value exceeding 200 mg/dl. They defined hyperglycemia as any value >200 mg/dl.
Glucose tolerance tests showed six patients with hyperglycemia, including five who had normal fasting levels. Furthermore, 26 additional patients were identified who had reactive hypoglycemia (low blood sugar) and another eight who had both low and high blood sugars.
The abnormal swings in blood glucose stimulated the researchers to comment that care must be taken when commenting that bariatric surgery can cure diabetes. In addition, this finding lends thought to what should be done in the future to better serve the needs of the bariatric population since the goal is to take weight off and keep it off while remaining healthy.
The findings suggest that alterations in the gastric bypass procedures need to be considered such as the use of valves or possibly using the vertical-sleeve gastrectomy and duodenal switches that are not as severely malabsorptive.


 Nutraceuticals are extracts from food that have shown purported medical and/or nutritional value. Occasionally, nutraceuticals are used in the form of food, but the amounts needed are often too great to achieve the benefits obtained from the isolated food extract.
Nutraceuticals are extracts from food that have shown purported medical and/or nutritional value. Occasionally, nutraceuticals are used in the form of food, but the amounts needed are often too great to achieve the benefits obtained from the isolated food extract.